
Rates of gestational diabetes in the United States have climbed steadily over the last decade, with a new analysis showing a 36% increase from 2016 to 2024. Researchers analyzing nearly 13 million first-time, single-baby birth records report growing incidence across all major racial and ethnic groups — but with pronounced differences in some populations. The trend raises urgent questions about prevention, equity in care, and long-term risks for parents and children.
What the data shows and why it matters
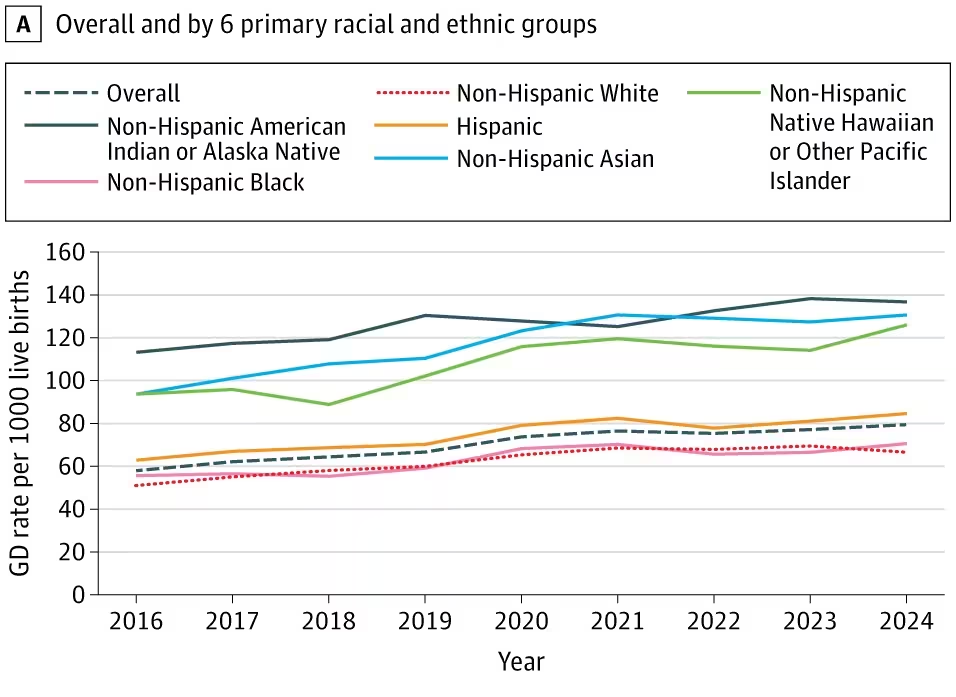
Northwestern University investigators used National Center for Health Statistics birth-certificate data for first births to calculate diagnoses of gestational diabetes when treatment for glucose intolerance was recorded. Across the combined nine-year period from 2016–2024, the team found an overall 36% rise in diagnoses: today, gestational diabetes affects roughly 79 out of every 1,000 first-time single births in the US.
The biological basis is straightforward but important to restate. During pregnancy the placenta produces hormones that can make maternal tissues less responsive to insulin, the hormone that moves sugar from blood into cells. In most pregnancies the pancreas compensates by producing extra insulin. Gestational diabetes occurs when that compensation is insufficient, leading to higher blood glucose. Elevated maternal glucose crosses the placenta, increasing fuel availability and sometimes prompting faster fetal growth — which can contribute to larger birth weight and delivery complications.
Longer-term consequences matter too: parents who develop gestational diabetes face a higher lifetime risk of type 2 diabetes, and children born after pregnancies complicated by gestational diabetes also carry increased metabolic risk later in life. Treatments depend on severity and individual factors and may include dietary changes, exercise, frequent blood-glucose monitoring, and insulin therapy when needed.
Unequal burden: who is most affected and possible drivers
The rise in gestational diabetes was seen across all racial and ethnic groups, but the rates are not evenly distributed. In 2024 the study reported particularly high diagnoses among American Indian/Alaska Native mothers (137 per 1,000 first births), Asian mothers (131 per 1,000), and Native Hawaiian/Pacific Islander mothers (126 per 1,000). These figures point to structural and biological drivers that deserve closer study.
Cardiologist Nilay Shah, a co-author of the study, notes: "Gestational diabetes has been persistently increasing for more than 10 years, which means whatever we have been trying to do to address diabetes in pregnancy has not been working." He and colleagues highlight several plausible contributors: differences in exposure to established risk factors (such as obesity and socioeconomic status), variations in health behaviors and access to prenatal care, and broader social determinants including discrimination in healthcare settings.
Past work covering 2011–2019 showed complex patterns. For example, some Asian subgroups exhibited high rates of gestational diabetes despite lower average body mass index and higher educational attainment, indicating that BMI alone does not explain the disparities. Other groups with higher average BMI or lower educational attainment showed elevated rates for more predictable reasons. This mix suggests that interventions must be tailored and informed by community-level data.
Policy and clinical implications
Researchers argue that public health and policy interventions should focus on ensuring access to high-quality prenatal care, culturally competent screening and treatment, and resources that enable people to adopt and maintain healthful behaviors before and during pregnancy. Early identification and appropriate management during pregnancy reduce immediate risks and could help prevent downstream type 2 diabetes.
The research, published in JAMA Internal Medicine, underscores the need for coordinated efforts across obstetrics, primary care, public health, and community organizations to reverse this trend. Better prevention strategies, improved access to healthful foods and safe exercise options, and unbiased clinical care are central to slowing — and ultimately reversing — the rise in gestational diabetes.

“My work centers on sustainability, energy, and environmental science — examining how innovation can lead to a greener future.”

Discussion
Leave a Comment