
No lungs. Forty-eight hours. A heart kept beating while a machine did the breathing work of both lungs.
In spring 2023 a 33-year-old man caught a flu that would not behave. The infection accelerated into pneumonia, then sepsis, and finally acute respiratory distress syndrome (ARDS) — a rapid collapse of the lungs' ability to exchange oxygen. Antibiotics failed. The lung tissue essentially liquefied, spreading inflammation through his body. The medical team faced a grim choice: leave the infected lungs in place and the patient would almost certainly die; remove them and the heart, starved of proper pulmonary circulation, could also fail.
Turning lungs into lungs-on-demand
Northwestern University’s surgeons answered the dilemma with a bold adaptation of extracorporeal support: a total artificial lung (TAL). Unlike standard extracorporeal membrane oxygenation (ECMO), which oxygenates blood but relies on existing pulmonary circuit dynamics, the TAL built by the team replicated pulmonary gas exchange while actively managing blood flow and protecting the heart.
The device combined two parallel blood-flow channels with a flow-adaptive shunt. The result was a system that could smooth out sudden shifts in circulation after both native lungs were removed — the key obstacle that usually makes bilateral pneumonectomy (removal of both lungs) fatal. With the lungs removed and the TAL in place, signs of systemic recovery from infection began within hours, not weeks.
"He had developed an infection of his lungs that just could not be treated with any antibiotics because it was resistant to everything," said thoracic surgeon Ankit Bharat, who led the procedure. "That infection caused his lungs to liquify and then continued to progress to the rest of his body." Molecular analysis of the excised lungs confirmed what the team suspected: the immune and fibrotic damage made spontaneous recovery impossible. Transplantation, not salvage, was the only realistic path to survival.
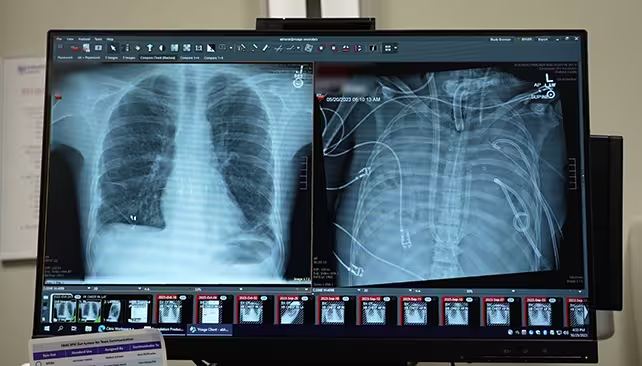
The patients' new lungs (left) and old lungs (right).
The TAL bought time. Enough time for the patient’s sepsis to come under control, for other organs to stabilize, and for use of a donor pair of lungs to become viable. After 48 hours on the TAL, surgeons performed a double lung transplant. Two years on, the patient has recovered and is living with functioning donor lungs.
Why this matters
ARDS from infections is often treated with aggressive supportive care, and many clinicians assume that if a patient is supported long enough the lungs will heal. This case challenges that assumption. It shows that, in selected patients with irreversible lung destruction from infection, removing the diseased organs and substituting a reliable artificial lung can be lifesaving — provided a transplant is available within a narrow window.
There are practical limits. Building and running a TAL of this complexity currently requires specialized surgical teams and engineering support available only at a few centers. Donor-lung availability also remains the rate-limiting step. Yet the innovations used here — particularly the dual-flow architecture and flow-adaptive shunt — could guide redesigns of extracorporeal devices used more broadly in intensive care units.
For young patients with catastrophic lung damage from infections, transplantation can be life-saving even in acute settings if surgical teams consider it and the infrastructure exists to support it.
Expert Insight
"This case reframes our thinking about acute lung failure," says Dr. Emily Carter, a cardiothoracic intensivist with long experience in mechanical circulatory support. "We used to reserve transplant for chronic, slowly progressive diseases. Now we see that, when infection destroys lung architecture beyond repair, temporary total artificial-lung support plus timely transplantation can — and should — be part of the conversation."
Beyond the immediate clinical triumph, the case pushes a broader technical agenda: make extracorporeal systems smarter about flow, reduce thrombosis risk, and design devices that intensive-care teams can deploy more widely. That will require engineering partnerships, regulatory pathways, and training programs to scale what is now a center-of-excellence capability.
Who benefits from that effort? Patients who today often have no options. Who pays? Health systems that must weigh short-term costs against lives saved and long-term recovery. The next step is expanding trials and reporting outcomes so that this approach moves from dramatic case report to validated treatment pathway — for the few who need it now and, perhaps, many more in the future.
It’s a reminder that medicine’s edges are where engineering, critical care, and surgical daring meet — and that sometimes survival means imagining an organ’s function long enough to replace it.

“My work centers on sustainability, energy, and environmental science — examining how innovation can lead to a greener future.”

Discussion
Leave a Comment