
Subtle changes in how older adults drive — fewer trips, simpler routes and less speeding — can be an early sign of cognitive decline. Recent research indicates that everyday driving patterns captured by GPS tracking devices, combined with standard cognitive tests, may help detect mild cognitive impairment (MCI) before crashes or overt symptoms emerge. By analyzing driving behavior as a real-world functional measure, clinicians and researchers hope to identify early warning signs that enable safer interventions, better care planning and preserved independence for older drivers.
How researchers turned GPS data into an early-warning signal
Researchers at Washington University in St. Louis followed volunteers for up to 40 months, automatically logging driving behavior with unobtrusive onboard GPS devices installed in participants' vehicles. The study cohort included 56 people previously diagnosed with mild cognitive impairment (MCI), a condition that often precedes Alzheimer’s disease, and 242 cognitively normal peers. The average age across participants was 75 years, reflecting a population at elevated risk for age-related cognitive change.
The team extracted continuous driving metrics such as trip frequency, trip distance, route complexity (measured by variability and route entropy), speeding per trip, and duration of longer journeys. These GPS-derived behavioral indicators were then statistically matched against established neuropsychological tests that assess memory, attention and executive function. Demographic and biological covariates — age, education, and presence of a known genetic Alzheimer’s risk marker — were included in predictive models to control for baseline differences.
Using combined inputs from GPS-derived driving information, clinical cognitive scores and demographic data, the researchers reported that their models could correctly identify cognitive decline among participants with preexisting MCI roughly 87% of the time. Models relying on driving data alone still detected MCI at about an 82% success rate. Those figures indicate that passive, continuous monitoring of driving behavior provides substantial incremental predictive value beyond single-point clinic tests and demographic risk factors.
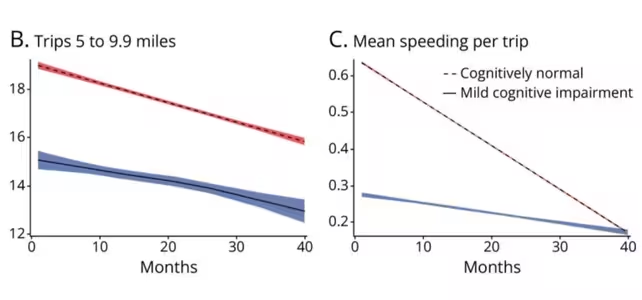
B) Longer trips and C) speeding per trip declined as measured over 40 months, comparing cognitively normal (red/dashed) with MCI (blue/solid) (Chen et al., Neurology, 2025)
What these driving patterns actually look like
Across the monitoring window, drivers with MCI displayed consistent behavioral changes: they made fewer overall trips, visited fewer unique destinations, and increasingly relied on familiar, simpler routes. Measures of risk-taking — such as speeding events per trip — and the time spent on longer journeys declined over time. These changes were gradual and often subtle, detectable only through continuous, objective logging rather than intermittent self-report or infrequent clinic assessments.
Some of the observed pattern shifts likely represent intentional self-regulation. Older adults commonly reduce driving exposure, avoid high-traffic or nighttime driving, and opt for shorter, routine errands as a personal safety strategy. However, the study’s strength lies in distinguishing self-regulation from cognitive-driven decline: the regular, quantifiable reductions in route complexity and trip variety correlated with declines on memory and executive function tests, suggesting a behavioral biomarker of underlying cognitive changes rather than solely voluntary lifestyle adjustments.
Technically, the driving metrics that showed the strongest associations with cognitive measures included:
- Trip frequency and daily driving exposure (total trips per week and average daily distance)
- Route complexity or entropy (variability of routes and number of unique destinations)
- Speeding and abrupt acceleration/braking events (indicators of situational awareness and motor control)
- Duration and frequency of longer journeys (reflecting planning, confidence and navigation ability)
Combining richer telematics — such as lane-keeping events, steering variability, or right-angle turns — with GPS-derived spatial metrics offers a more complete picture of on-road performance and may improve early detection. Importantly, the metrics used in this study are low-burden and can be passively collected without active engagement from participants, increasing feasibility for long-term monitoring.
Why this matters for safety, diagnosis and care planning
Driving is a complex daily activity that requires intact spatial navigation, decision-making, divided attention and sensorimotor coordination. Small declines across these cognitive domains can change driving behavior well before standard clinic-based cognitive tests register measurable impairment. Detecting those patterns earlier creates opportunities to intervene: targeted driving assessments, road-safety counseling, adaptive technologies (such as route guidance or driver assistance), and care planning can be introduced earlier to reduce crash risk and preserve mobility safely.
From a public health and clinical standpoint, the ability to identify early functional decline using GPS tracking has several practical advantages:
- Early intervention: Timely referrals to occupational therapists or driving rehabilitation programs can be arranged before incidents occur.
- Personalized risk communication: Families and clinicians can make informed, individualized plans about driving restrictions or alternatives like ride services and community transport.
- Resource prioritization: Health systems can triage higher-risk individuals for comprehensive cognitive evaluations, neuroimaging, or medication reviews.
- Longitudinal monitoring: Passive data allow clinicians to observe trends over months to years rather than relying on single time-point assessments.
Researchers emphasize that GPS monitoring is not a standalone diagnostic tool. Rather, it can augment routine clinical evaluations as a behavioral biomarker that flags individuals who may benefit from in-depth cognitive testing or targeted safety interventions. Integrating GPS-derived analytics into clinical workflows could form part of a multi-modal assessment strategy that combines neuropsychological testing, caregiver reports, and functional measures to refine diagnosis and management of MCI and early Alzheimer’s disease.
Legal, insurance and ethical implications must be considered. Continuous behavioral monitoring raises questions about consent, data ownership, reporting responsibilities, and potential misuse (for example, by insurers or licensing authorities). The study authors and ethicists advocate for transparent consent processes, clear data governance policies, and safeguards that prioritize the autonomy and dignity of older drivers while balancing road safety concerns.
Next steps: bigger studies and broader data
To evaluate generalizability, the Washington University team plans to validate the approach in larger, more diverse populations and to incorporate additional contextual variables. Future work will examine how vehicle type (car size, safety features), geographic driving environment (urban vs. suburban vs. rural), local traffic patterns, and comorbid medical conditions (e.g., visual impairment, Parkinsonian signs, cardiovascular disease) interact with driving-derived signals of cognitive decline.
Key validation tasks include:
- Expanding sample diversity: Recruit participants across different ages, racial and ethnic backgrounds, and socioeconomic strata to test model performance across populations.
- Algorithm refinement and external validation: Use independent datasets to assess sensitivity, specificity and predictive value, and minimize biases in machine-learning models.
- Contextual feature integration: Incorporate accelerometer, camera, or advanced telematics data where feasible to enrich behavioral markers while balancing privacy concerns.
- Clinical pathway development: Define how GPS-derived alerts are delivered to clinicians, what follow-up assessments are triggered, and how families are engaged in a supportive, non-punitive way.
Broader testing will help determine whether the signals observed in this cohort generalize across different driving cultures, regulatory contexts and levels of digital access. For example, older adults in dense urban centers may show different route variability patterns than those in rural areas where travel distances and road types vary widely. Similarly, disparities in smartphone or vehicle telematics adoption could affect data completeness and model equity, so inclusive deployment strategies are essential.
Expert Insight
Neurology researcher Ganesh Babulal emphasized the public health importance of early detection: "Early identification of older drivers who are at risk for accidents is a public health priority, but identifying people who are unsafe is challenging and time-consuming. We found that using a GPS data tracking device, we could more accurately determine who had developed cognitive issues than by looking only at age, cognitive test scores, and a genetic risk marker related to Alzheimer’s disease." His comments underscore how real-world, continuous measures of function can complement clinical data to improve risk stratification.
Dr. Elena Morris, a cognitive neuroscientist specializing in aging and mobility, adds a practical perspective: "Behavioral signals like driving patterns are powerful because they capture function in the real world. Clinic tests are essential, but they only provide a snapshot. Continuous, passive monitoring can reveal trends before a crisis — as long as we protect privacy and use the data to support, not punish, older adults." Dr. Morris highlights the ethical imperative to design monitoring programs that enhance safety and autonomy rather than restrict freedoms unnecessarily.
Technically, translating this research into clinical practice will require interoperable systems and clear standards for data quality, consent and interpretability. Developers should aim for transparent machine-learning models whose decision rules can be explained to clinicians and participants. Thresholds for alerts should be evidence-based and tuned to minimize false positives that could lead to unwarranted restrictions, while preserving sensitivity to meaningful decline.
Finally, integrating GPS-derived driving metrics with traditional cognitive screening, caregiver reports and medical history could create a more sensitive, ethical and actionable pathway for early detection of cognitive decline. Doing so would give clinicians, families and drivers more time to plan, adapt and stay safer on the road, while opening pathways to research on interventions that preserve mobility and quality of life as cognition changes.
As the field advances, multi-disciplinary collaboration among neurologists, geriatricians, occupational therapists, data scientists, ethicists and policymakers will be essential to realize the potential of driving behavior as a scalable, real-world biomarker for mild cognitive impairment and early Alzheimer’s disease.

“The cosmos has always fascinated me. I write about space missions, astronomy, and the technologies pushing humanity beyond Earth.”

Discussion
Leave a Comment