
A long-running shingles vaccination program in Wales has produced surprising and potentially important results: researchers now link the zoster jab not only to fewer new dementia cases but also to slower cognitive decline and reduced dementia-related mortality in people already diagnosed. These observations add to growing evidence that vaccines targeting nervous-system viruses could become part of dementia prevention and care strategies, alongside existing lifestyle and vascular-risk interventions.
A real-world program turned into a natural experiment
When the UK National Health Service rolled out a shingles vaccine program in Wales in 2013, what seemed like a routine implementation decision created a rare natural experiment for epidemiologists and public-health researchers. To prioritize distribution, the program invited people born in a specific year—age 79 at the time—while excluding those who had just turned 80. That single-year cutoff produced two cohorts separated by only one year of age but otherwise similar with respect to many background characteristics.
Because age is a dominant risk factor for dementia, the narrow age window minimized confounding by long-term socioeconomic and educational differences that often complicate observational research. In effect, the policy-created cutoff functioned like an unplanned randomized allocation in a real-world population, allowing scientists to compare outcomes for vaccinated and unvaccinated groups with improved internal validity compared with standard retrospective comparisons.
Using linked electronic health records, an international team of researchers examined outcomes for tens of thousands of older adults exposed to the Welsh rollout. They focused on both incidence—new diagnoses of mild cognitive impairment (MCI) and dementia—and progression and mortality among people with preexisting dementia. In a subgroup of 14,350 people who already had a dementia diagnosis before the program began, those who received the shingles vaccine had an almost 30 percent lower risk of dying of dementia over the subsequent nine years than their slightly older, unvaccinated peers. At the same time, the broader dataset reinforced earlier signals connecting shingles vaccination with lower rates of MCI and fewer new dementia diagnoses overall.
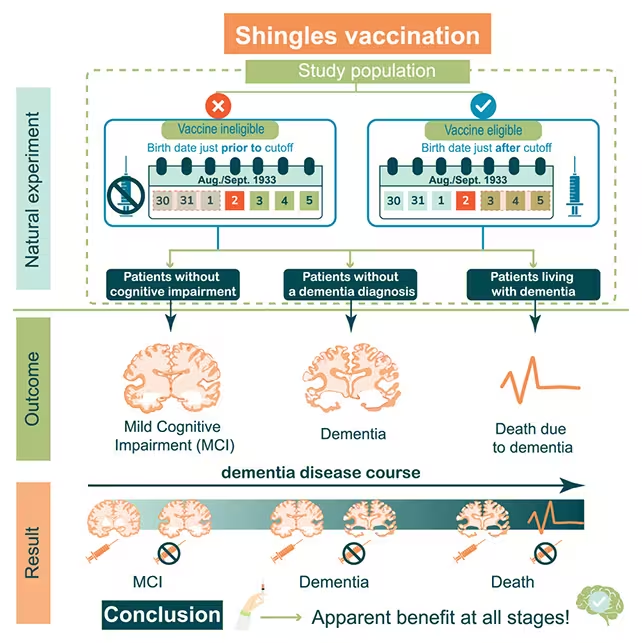
The vaccine protected against dementia and mild cognitive impairment.
Why this matters: prevention and possible treatment
Most dementia research has emphasized primary prevention or early intervention to slow decline before a clinical diagnosis. These new observations suggest the shingles vaccine might have dual utility: it may reduce the risk of developing cognitive impairment and also temper decline and mortality for people who already have dementia. That combination—both preventive and therapeutic potential—carries important public-health implications because the vaccine used in Wales is inexpensive, has a well-established safety profile, and is already available through routine immunization programs in many countries.
From a population-health perspective, a low-cost intervention that lowers incidence and reduces mortality among people living with dementia would shift preventive planning and resource allocation. Dementia imposes substantial clinical and economic burdens on health systems and caregivers; any intervention that reduces new cases or slows progression could impact care planning, long-term costs, and quality of life for patients and families.
Cardiff University epidemiologist Haroon Ahmed emphasizes that existing safety data and broad availability make this an especially promising line of inquiry. Yet researchers caution that observational studies cannot by themselves prove causation. The Welsh rollout provided a quasi-experimental design by accident, but carefully controlled clinical trials and mechanistic studies will be needed to confirm whether the association is causal and to measure the magnitude and duration of any protective effect.
Possible biological mechanisms
Scientists are exploring several plausible biological explanations for the observed association between shingles vaccination and lower dementia risk or slower progression. Shingles is caused by reactivation of the varicella zoster virus (VZV), which initially causes chickenpox and then can remain dormant in sensory ganglia for decades. Reactivation of VZV in nervous tissue can cause local inflammation, neuronal injury, and peripheral neuropathic pain; researchers are now investigating whether repeated or subtle viral reactivation in older adults might contribute to neurodegenerative cascades.
Animal models and neuropathology studies suggest that viral activity in nervous tissue may promote accumulation of abnormal proteins—such as amyloid-beta and tau aggregates—that are characteristic of Alzheimer’s disease and other neurodegenerative conditions. Viral proteins or virus-induced immune responses might accelerate protein misfolding, synaptic dysfunction, or neuronal loss. If vaccination reduces viral reactivation, it could indirectly slow processes that eventually culminate in cognitive decline.
Another set of hypotheses centers on immune modulation. Aging is associated with changes in the innate and adaptive immune systems—sometimes referred to as immunosenescence—which can increase susceptibility to infections and alter inflammatory responses. Vaccination stimulates immune memory and may reduce the frequency of subclinical reactivations, lowering chronic neuroinflammation. Chronic neuroinflammation is increasingly seen as a contributor to neurodegeneration; thus a vaccine-induced reduction in inflammatory episodes could plausibly slow disease progression.
Some investigators also propose broader, non-specific effects of vaccination. Certain vaccines can produce systemic immune adaptations or trained immunity that influence responses to other pathogens or inflammatory insults. While the mechanisms of trained immunity remain under investigation, this concept has been invoked to explain unexpected broader health benefits observed with some immunizations. Clarifying whether shingles vaccination exerts virus-specific effects, immune-modulatory effects, or a combination of both will require laboratory studies, longitudinal biomarker collection, and randomized clinical trials that include imaging and fluid markers of neurodegeneration.
What researchers want to test next
- Expand analyses to larger, multiethnic, and international populations across different age ranges to assess the consistency and generalizability of the protective signal in diverse health systems and demographic groups.
- Compare the older live-attenuated vaccine formulation used in early rollouts with newer, recombinant subunit shingles vaccines to determine whether updated formulations provide similar or stronger protection against cognitive decline and dementia-related outcomes.
- Design prospective clinical trials or nested cohort studies that collect biological samples (blood, cerebrospinal fluid), imaging (MRI, PET), and standardized cognitive assessments to probe mechanisms: document viral reactivation, profile immune-state changes, and measure protein aggregation biomarkers over time.
- Assess dose–response relationships and timing effects: whether vaccination earlier in late midlife versus later in life yields different effects on dementia risk, and whether booster doses influence long-term outcomes.
In practical terms, investigators plan to use a combination of observational, mechanistic, and interventional approaches. For example, randomized controlled trials could enroll people at high risk for neurodegenerative disease or those already diagnosed with mild dementia to test whether shingles vaccination slows cognitive decline compared with placebo or standard care. Parallel laboratory studies using animal models can test causal pathways, such as whether VZV reactivation directly increases amyloid deposition or whether vaccine-induced changes in cytokine profiles mediate protective effects.
Pascal Geldsetzer, a biomedical scientist at Stanford University, described the results as encouraging because they hint at therapeutic potential for people already living with dementia. He and other authors argue the findings justify allocating research resources to investigate pathways that might connect herpesvirus activity, immune responses, and neurodegeneration. Strategic prioritization could accelerate translational studies that move from epidemiological association to clinical application.
Public-health implications and caution
If future controlled trials confirm a causal effect, shingles vaccination could become a low-cost, scalable component of dementia risk reduction strategies. It could complement interventions that address vascular risk factors (hypertension, diabetes, hyperlipidemia), social and cognitive engagement, physical activity, and diet. Because shingles vaccines are already licensed and distributed in many regions, integration into public-health guidance could be more rapid than for novel pharmaceutical agents—but only after sufficient evidence accumulates to justify policy change.
For clinicians and policymakers, the current evidence should be interpreted as promising but preliminary. Observational links can suggest hypotheses and identify interventions worth testing, but they do not establish definitive clinical guidance. The Welsh analysis reduces several common confounders through its quasi-experimental design, yet residual confounding or selection biases cannot be excluded. For example, people who accept vaccination may differ systematically in health-seeking behavior, comorbidity management, or access to care in ways that influence dementia outcomes.
Therefore, professional organizations and public-health agencies must balance enthusiasm with rigorous evaluation. Recommendations to prioritize shingles vaccination primarily for dementia prevention would be premature today; instead, findings should motivate targeted randomized trials, mechanistic research, and cost-effectiveness modeling to determine whether the observed associations translate into actionable policy.
Expert Insight
Dr. Maya Reed, a neurologist focused on neuroinfectious disease, offers a practical perspective: "These results are a reminder that infections and immunity matter for brain health. A widely available vaccine that reduces not only incidence but also mortality from dementia would be a game-changer—but we must test it carefully. The next steps are controlled trials and biomarker work to show whether the effect is direct or mediated through reduced inflammation or viral suppression."
Experts also emphasize the value of interdisciplinary collaboration. Understanding whether shingles vaccination affects dementia risk will require clinicians, epidemiologists, virologists, immunologists, neuropathologists, and health economists working together. Cross-disciplinary studies can integrate population-level evidence with mechanistic insights—accelerating translation from epidemiological signal to clinical recommendation if the evidence supports it.
Operationally, researchers recommend creating pre-specified analysis plans, registering trials, and sharing de-identified data and protocols to improve reproducibility. They also suggest stratified analyses that consider comorbidities (for example, cardiovascular disease or immunosuppressive therapies), genetic risk factors (such as APOE genotype), and socioeconomic determinants to ensure findings apply across subgroups and to identify populations most likely to benefit.
In short, the Welsh program provided scientists with a valuable, though imperfect, lens on how vaccines might influence brain aging. The accumulated evidence now calls for deliberate, well-funded follow-up studies to determine whether a familiar, widely available vaccine could play a new role in the global effort to prevent and treat dementia. Until then, clinicians should continue to follow established immunization guidelines and manage dementia risk using evidence-based lifestyle and medical approaches.

“My work centers on sustainability, energy, and environmental science — examining how innovation can lead to a greener future.”

Discussion
Leave a Comment